VEMLIDY optimizes tenofovir delivery to the hepatocyte1-6
VEMLIDY demonstrates enhanced plasma stability vs TDF for more efficient delivery of tenofovir to hepatocytes1-6
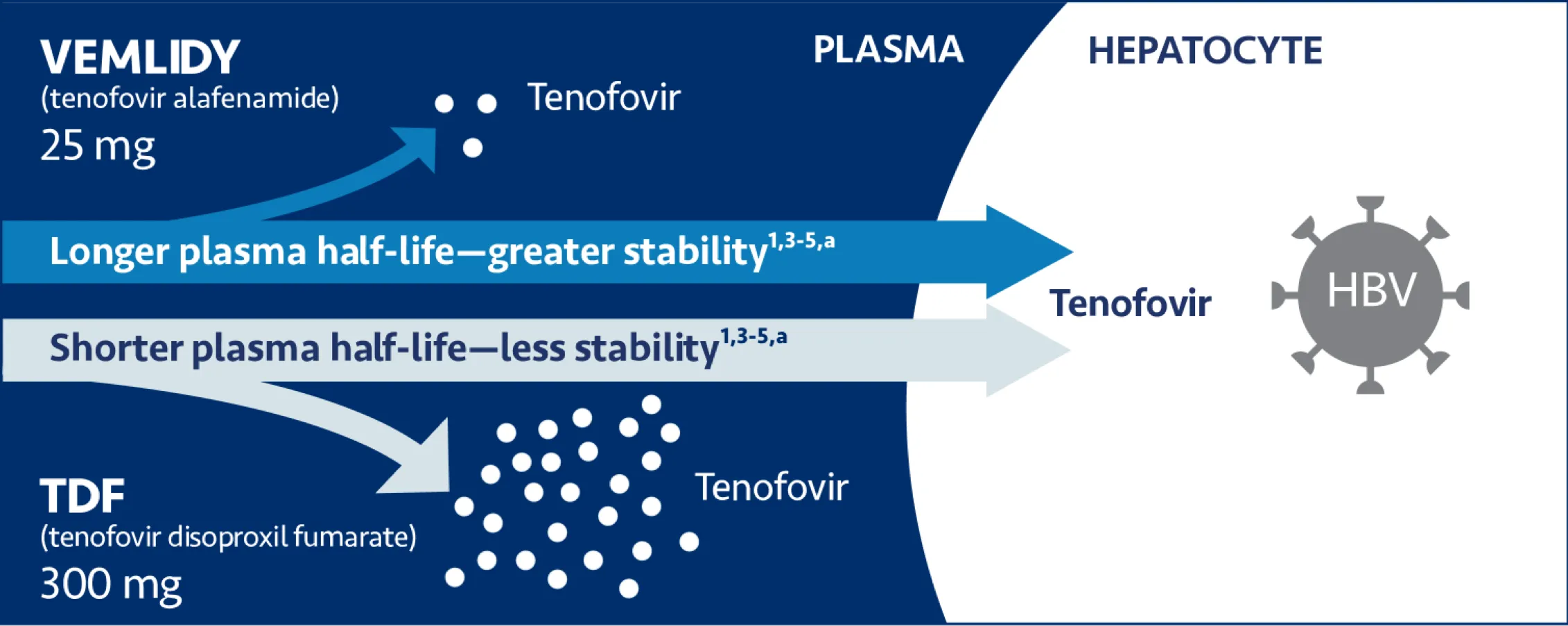
TDF=tenofovir disoproxil fumarate.
a Plasma half-life: VEMLIDY=30.6 minutes (0.51 hour)1; TDF=0.41 minutes.1,5
VEMLIDY is a novel, targeted prodrug of tenofovir
Why a prodrug?
- Tenofovir does not readily cross cell membranes and is poorly absorbed after oral administration due to 2 negative charges on the molecule7,8
- Prodrugs of tenofovir are required for better absorption7
- Both VEMLIDY and TDF are prodrugs of tenofovir and have demonstrated increased cellular permeability and oral bioavailability compared with tenofovir7,8
VEMLIDY provides greater plasma stability than TDF
- VEMLIDY is a novel, targeted phosphonamidate prodrug of tenofovir1
- TDF is an ester prodrug5
- The phosphonamidate group provides greater plasma stability in VEMLIDY than TDF1,3,4,6
How does VEMLIDY compare to TDF?
- VEMLIDY breaks down less readily in the plasma than TDF for more efficient drug delivery into the hepatocytes1,3,4,6
- 89% less tenofovir in the plasma than TDF allows for VEMLIDY to be given at approximately 1/10th the dose of TDF1-3,5
Warnings and Precautions
- Risk of Development of HIV-1 Resistance in HBV/HIV-1 Coinfected Patients: Due to this risk, VEMLIDY alone should not be used for the treatment of HIV-1 infection. Safety and efficacy of VEMLIDY have not been established in HBV/HIV-1 coinfected patients. HIV antibody testing should be offered to all HBV-infected patients before initiating therapy with VEMLIDY, and, if positive, an appropriate antiretroviral combination regimen that is recommended for HBV/HIV-1 coinfected patients should be used.
References: 1. VEMLIDY Prescribing Information. Foster City, CA: Gilead Sciences, Inc.; March 2024.
2. TDF (tenofovir disoproxil fumarate) Prescribing Information. Gilead Sciences, Inc.; April 2019. 3. Chan HLY, Fung
S, Seto WK, et al; GS-US-320-0110 investigators. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the
treatment of HBeAg-positive chronic hepatitis B virus infection: a randomised, double-blind, phase 3,
non-inferiority trial. Lancet Gastroenterol Hepatol. 2016;1(3):185-195. doi:10.1016/S2468-1253(16)30024-3 4. Agarwal
K, Fung SK, Nguyen TT, et al. Twenty-eight day safety, antiviral activity, and pharmacokinetics of tenofovir
alafenamide for treatment of chronic hepatitis B infection. J Hepatol. 2015;62(3):533-540.
doi:10.1016/j.jhep.2014.10.035 5. Lee WA, He GX, Eisenberg E, et al. Selective intracellular activation of a novel
prodrug of the human immunodeficiency virus reverse transcriptase inhibitor tenofovir leads to preferential
distribution and accumulation in lymphatic tissue. Antimicrob Agents Chemother. 2005;49(5):1898-1906.
doi:10.1128/AAC.49.5.1898-1906.2005 6. Murakami E, Wang T, Park Y, et al. Implications of efficient hepatic delivery
by tenofovir alafenamide (GS-7340) for hepatitis B virus therapy. Antimicrob Agents Chemother. 2015;59(6):3563-3569.
doi:10.1128/AAC.00128-15 7. Ray AS, Fordyce MW, Hitchcock MJ. Tenofovir alafenamide: a novel prodrug of tenofovir
for the treatment of Human Immunodeficiency Virus. Antiviral Res. 2016;125:63-70. 8. Lou L. Advances in nucleotide
antiviral development from scientific discovery to clinical applications: tenofovir disoproxil fumarate for
hepatitis B. J Clin Transl Hepatol. 2013;1:33-38. 9. Data on file. Gilead Sciences, Inc. 10. Ghany MG, Pan CQ, Lok AS, et al. AASLD IDSA Practice Guideline on treatment of chronic hepatitis B. Hepatology. 2026;83(4):974-997. doi:10.1097/HEP.0000000000001549 11. You H, Wang F, Li T, et al. Guidelines for the prevention and
treatment of chronic hepatitis B (version 2022). J Clin Transl Hepatol. 2023;11(6):1425-1442.
doi:10.14218/JCTH.2023.00320 12. Tong MJ, Pan CQ, Han SB, et al. An expert consensus for the management of chronic
hepatitis B in Asian Americans. Aliment Pharmacol Ther. 2018;47:1181-1200. 13. Martin P, Nguyen MH, Dieterich DT, et
al. Treatment algorithm for managing chronic hepatitis B virus infection in the United States: 2021 update. Clin
Gastroenterol Hepatol. 2021;S1542-3565(21)00818-1. doi:10.1016/j.cgh.2021.07.036 14. European Association for the
Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol.
2025;83(2):502-583. doi:10.1016/j.jhep.2025.03.018
15. Dieterich D, Graham C, Wang S, et al. It is time for a simplified approach to hepatitis B elimination. Gastro Hep Adv. 2022;2(2):209-218. doi:10.1016/j.gastha.2022.10.004