VEMLIDY was proven in robust, global clinical trials
The efficacy and safety profile of VEMLIDY in the treatment of adults with chronic hepatitis B infection with compensated liver disease was based on data from 3 randomized, double-blind, active-controlled trials with 1786 patients (HBeAg– and HBeAg+)1-3,a
a Study 4018 included 488 virologically suppressed patients; Study 108 included 425 HBeAg− patients; Study 110 included 873 HBeAg+ patients.
Pivotal trials and open-label extension (OLE): 108 and 110
~75% of patients enrolled in pivotal trials 108/110 were treatment-naïve2
The efficacy and safety of VEMLIDY in the treatment of adults with chronic HBV infection with compensated liver disease are based on data from 2 randomized, double-blind, active-controlled, noninferiority trials.1,4-7,b
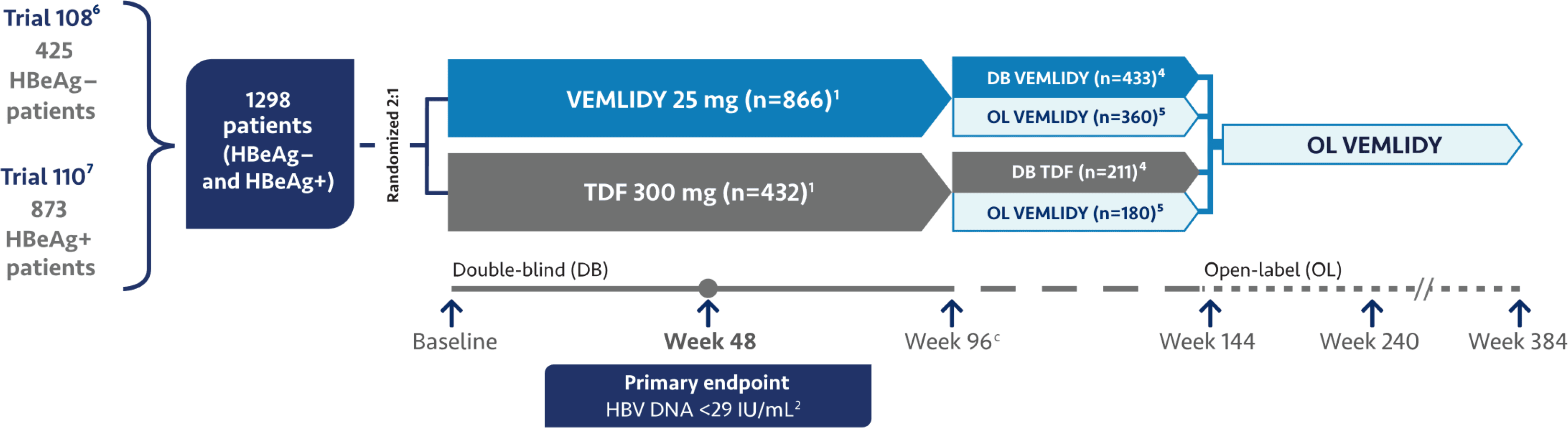
b Key inclusion criteria: HBV DNA ≥20,000 IU/mL; ALT >60 U/L (males) or >38 U/L (females) and ≤10x ULN by central laboratory range.6,7
c The numbers of patients listed after Week 96 refer to those who entered the open-label phase or remained in the double-blind phase and exclude patients who prematurely discontinued double-blind study treatment by Week 96.4,5
Trial 108 (N=425)1
- HBeAg- patients (79% treatment-naïve patients, 21% treatment-experienced patients)1,4
Trial 110 (N=873)1
- HBeAg+ patients (74% treatment-naïve patients, 26% treatment-experienced patients)1,4
The primary endpoint for both studies was HBV DNA <29 IU/mL and noninferiority to TDF (10% margin; 95% confidence interval [CI] approach) at Week 48.6,7
Additional efficacy endpoints evaluated at Week 48, Week 96, and Week 144 for both trials included the proportion of patients with1,4,6:
- HBV DNA <29 IU/mL
- ALT normalization
- HBsAg loss and seroconversion
HBeAg loss and seroconversion were also assessed in Trial 110.1
The original protocol was amended to extend the double-blind phase from 96 weeks to 144 weeks. However, before implementation of the protocol amendment, 540 patients entered the open-label phase at Week 96 (360 patients remained on VEMLIDY and 180 patients switched from TDF to VEMLIDY).4
By Week 144, a total of 1157 patients had entered the open-label phase.2
At Week 384, the full analysis set included 1298 patients who were enrolled in the study.2
The 8-year analysis is not presented in the VEMLIDY full Prescribing Information.
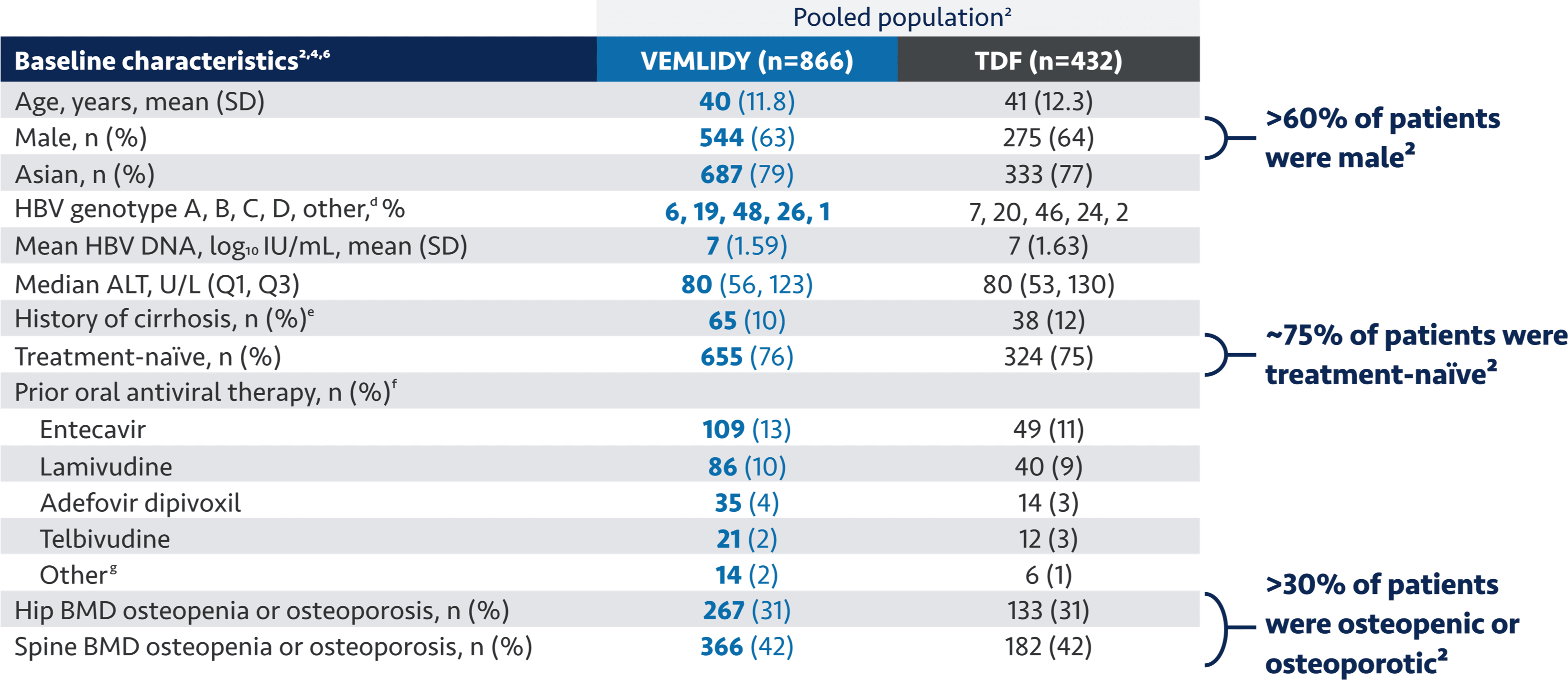
Treatment-naïve patients had <12 weeks of previous treatment with any nucleoside/nucleotide analog. Treatment-experienced patients met all entry criteria (including HBV DNA ≥20,000 IU/mL and serum ALT criteria) and
had ≥12 weeks of previous treatment with any nucleoside/
nucleotide analog.1,4
ALT=alanine aminotransferase; BMD=bone mineral density; HBeAg=hepatitis B envelope antigen; HBsAg=hepatitis B surface antigen; SD=standard deviation; TDF=tenofovir disoproxil fumarate; ULN=upper limit of normal.
d“Other” includes genotypes E, F, H, and unknown.2
eExcludes patients with missing values.2
f Excluding interferon and TDF. Patients may have been on more than one prior therapy.4
g “Other” category included clevudine, tenofovir alafenamide, and other oral nucleoside/nucleotide agents.4
Warnings and Precautions
- New Onset or Worsening Renal Impairment: Postmarketing cases of renal impairment, including acute renal failure, proximal renal tubulopathy (PRT), and Fanconi syndrome have been reported with TAF-containing products. Patients with impaired renal function and/
or taking nephrotoxic agents (including NSAIDs) are at increased risk of renal-related adverse reactions. Discontinue VEMLIDY in patients who develop clinically significant decreases in renal function or evidence of Fanconi syndrome. Monitor renal function in all patients –
See Dosage and Administration.