VEMLIDY: A demonstrated renal safety profile through 8 years1,2
Across multiple trials, VEMLIDY demonstrated a reduced effect on renal safety parameters and improved renal function when compared to baseline1,2
Change in eGFRCG from baseline to Week 96 (including open-label treatment after Week 48)3,4
Change in eGFRCG from baseline to Week 963
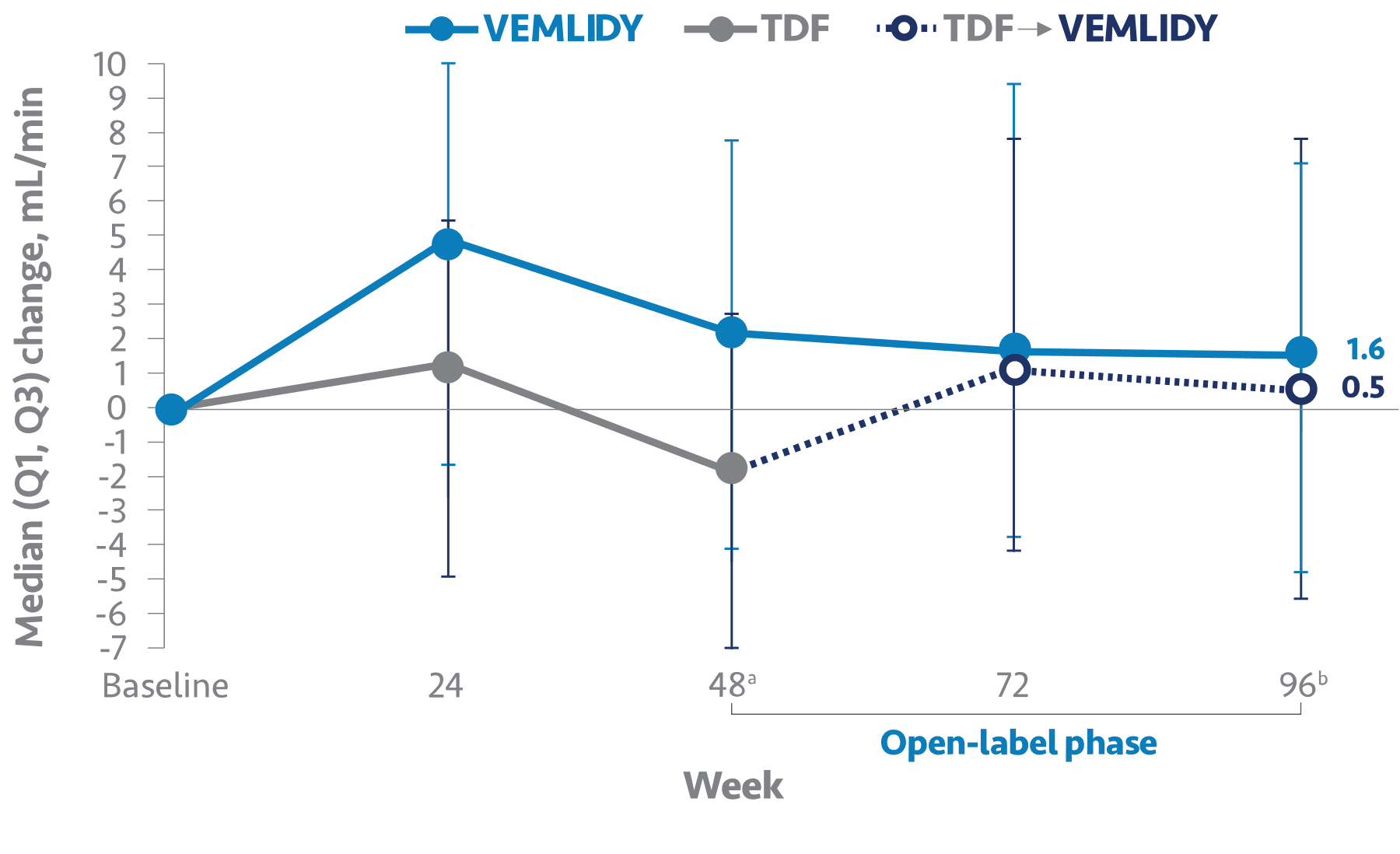
eGFRCG=estimated glomerular filtration rate by Cockcroft-Gault method, also referred to as eCrCl (estimated creatinine clearance); TDF=tenofovir disoproxil fumarate.
a P<0.0001; fallback procedure confirmed statistical significance using the adjusted alpha.3
bP=Not significant.3
- Median change from baseline to Week 48 in eGFRCG was +0.9 mL/min in the VEMLIDY group (n=243) and -2.7 mL/min in the TDF group (n=245)4
- Median baseline eGFRCG was 90.9 mL/min and 90.3 mL/min, for VEMLIDY and TDF, respectively4
The long-term clinical significance of these renal laboratory changes on adverse reaction frequencies between VEMLIDY and TDF is not known.1
Warnings and Precautions
- New Onset or Worsening Renal Impairment: Post marketing cases of renal impairment, including acute renal failure, proximal renal tubulopathy (PRT), and Fanconi syndrome have been reported with TAF-containing products. Patients with impaired renal function and/or taking nephrotoxic agents (including NSAIDs) are at increased risk of renal-related adverse reactions. Discontinue VEMLIDY in patients who develop clinically significant decreases in renal function or evidence of Fanconi syndrome. Monitor renal function in all patients – See Dosage and Administration.
References: 1. VEMLIDY Prescribing Information. Foster City, CA: Gilead Sciences, Inc.; March 2024. 2. Buti M, Lim YS, Chan HLY, et al. Eight-year efficacy and safety of tenofovir alafenamide for treatment of chronic hepatitis B virus infection: final results from two randomised phase 3 trials. Aliment Pharmacol Ther. 2024;60(11-12):1573-1586. doi:10.1111/apt.18278 3. Data on file. Gilead Sciences, Inc. 4. Lampertico P, Buti M, Fung S, et al. Switching from tenofovir disoproxil fumarate to tenofovir alafenamide in virologically suppressed patients with chronic hepatitis B: a randomised, double-blind, phase 3, multicentre non-inferiority study. Lancet Gastroenterol Hepatol. 2020;5(5):441-453. doi:10.1016/j.jhep.2017.11.039