VEMLIDY—proven long-term viral suppression in chronic hepatitis B patients with compensated liver disease1,2
Powerful efficacy maintained over the long term with 0% resistance2
Viral suppression at Weeks 48 and 961,3,4,a,b
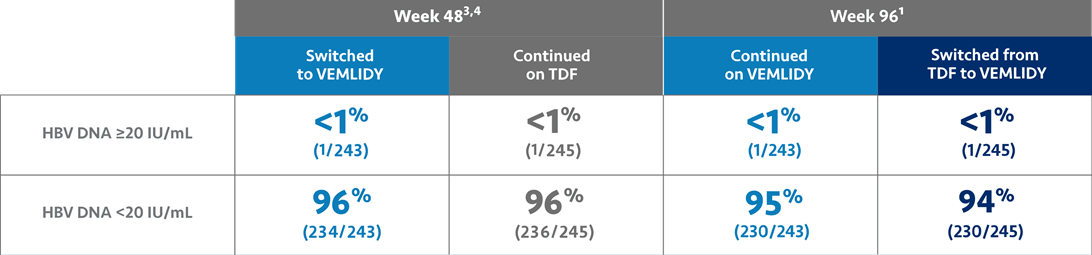
At Week 48, all patients who were in the TDF group in the controlled phase of the trial were switched to VEMLIDY which they used through Week 96 as part of the open-label extension phase. Patients who were originally assigned to VEMLIDY continued using it through Week 96.4
Adverse reactions observed with VEMLIDY in Trial 4018 were similar to those in Trials 108 and 110. Most common adverse reactions (incidence ≥5%, all grades) were headache, abdominal pain, cough, back pain, fatigue, nausea, arthralgia, diarrhea, and dyspepsia.1
The percentage of patients with no virologic data was 5% in the Continued on VEMLIDY group (n=12/243) and 6% in the Switched from TDF to VEMLIDY group (n=14/245) at Week 96.4
HBeAg=hepatitis B envelope antigen; TDF=tenofovir disoproxil fumarate.
aAt baseline, median duration of prior TDF treatment was 220 weeks (VEMLIDY) and 224 weeks (TDF).1
bNo patient discontinued treatment due to lack of efficacy. Treatment difference was adjusted by baseline age groups (<50 years, ≥50 years) and baseline HBeAg status strata. At Weeks 48 and 96, Trial 4018 had only 1 patient in each treatment group who had HBV DNA ≥20 IU/mL. Trial 4018 met the primary endpoint of noninferiority.1,4
See efficacy data from the pivotal trials.
Genotypic resistance analysis was performed on patients experiencing HBV DNA ≥69 IU/mL at any study visit through Week 96.1
Warnings and Precautions
- Risk of Development of HIV-1 Resistance in HBV/HIV-1 Coinfected Patients: Due to this risk, VEMLIDY alone should not be used for the treatment of HIV-1 infection. Safety and efficacy of VEMLIDY have not been established in HBV/HIV-1 coinfected patients. HIV antibody testing should be offered to all HBV-infected patients before initiating therapy with VEMLIDY, and, if positive, an appropriate antiretroviral combination regimen that is recommended for HBV/HIV-1 coinfected patients should be used.